


From Interprofessional Education to Collaborative Practice
6-7 Minutes
Author: Julpohng “JP” Vilai, MD, FAAP
Purpose
To familiarize clinicians with and provide resources for interprofessional education and collaborative practice.
Learning Objectives
1. Describe the current landscape of interprofessional practice and education;
2. Provide two examples of interprofessional learning modalities; and
3. Discuss ways for clinical educators to promote interprofessional practice and education.

In 1993, the American Nurses Association designated May 6-12 as permanent annual dates to observe National Nurses Week, culminating on May 12 to recognize Florence Nightingale’s birthday. Perhaps not coincidentally, May 6-10 is also Teacher Appreciation Week. As I recall my time as a clinical educator in a Montana private practice, I became aware that learners in rural communities struggled to find rotations that would fulfill their program requirement, especially in Pediatrics. Outpatient clinicians were reluctant to work with medical students, let alone other health professional students. Our clinic received dozens of pleading requests per month, but we were forced to decline many of them as only one other physician in my practice accepted non-medical students.

I often precepted nurse practitioner and physician assistant students concurrently with medical students and residents; sometimes my nurse also had a nursing student with her. Learners were encouraged to discuss patients and formulate management plans among themselves, and I would debrief and teach in groups that included all learners. I discovered that each profession, while having different approaches, contributed ideas and perspectives that generally enhanced the patient’s experience, and most learners were incredibly grateful for the educational opportunity. However, I recall being stunned by a medical student’s comment on one of my teaching evaluations expressing resentment about sharing the learning environment with a nurse practitioner student. While I was not yet aware that interprofessional practice and education was gaining national traction, this was an unexpected but formative introduction not only to the merits of interprofessional education but also its challenges.
The Past, Present, and Future of Interprofessional Practice and Education
Health care in the United States has become more complex and team-based with greater attention to prevention and social determinants of health.(1) As a result of this expanded definition of health, and recognizing that achieving this vision often requires collaboration of stakeholders, new models of interprofessional education and collaborative practice have emerged.(2,3) Importantly, evidence suggests an increased focus on interprofessional education (IPE) within required curricula,(4) and representatives from the nursing profession, in particular, have been instrumental in advancing interprofessional practice and education.(5)
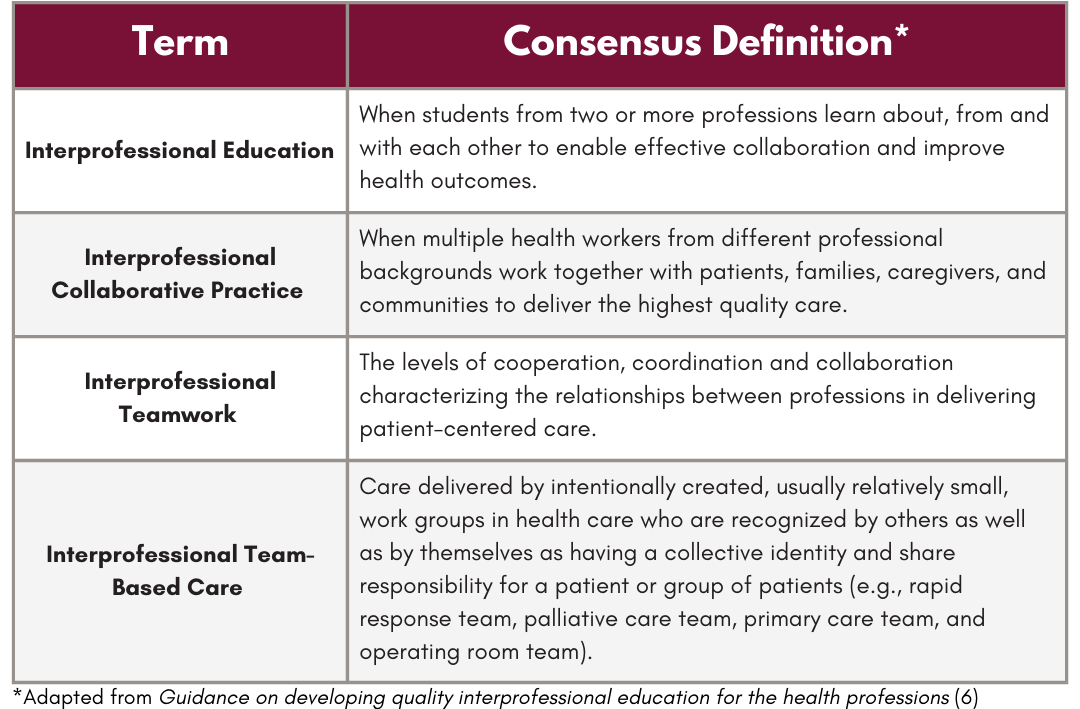
Whereas the abbreviation IPE has traditionally referred to InterProfessional Education, focused primarily on foundational and graduate medical education,(6,7) the concept of Interprofessional Practice and Education (the “new” IPE) was introduced in 2012 by the National Center for Interprofessional Practice and Education (hereafter, National Center)—a resource for expert guidance on IPE.(2,6) This vision reinforces that learning and practice are inseparable and that influencing health care and health systems must go beyond simply preparing learners to be collaborative.(8)
The Nexus Vision and Quadruple Aim Outcomes
In order to align interprofessional education and collaborative practice, the National Center presented the Nexus vision, “designed to intentionally link the health professions education and healthcare systems for interprofessional workforce development of future and current health professionals to simultaneously demonstrate organizational, learning and health outcomes.”(8,9)
The Nexus vision moves from primarily priming students for collaboration readiness to a partnership between education and health systems to impact individuals in real-time.(9) This impact has been articulated by the National Center as the Quadruple Aim outcomes: population health, patient experience, per capita cost, and provider work-life balance.(8,10) The primary goal of the Nexus vision is to improve Quadruple Aim outcomes.

Core Competencies for Interprofessional Collaborative Practice
With the purpose of defining interprofessional competencies that would prepare future health professionals for team-based care and improved health outcomes, six founding professional educational organizations (dentistry, nursing, medicine, osteopathic medicine, pharmacy, and public health) formed the Interprofessional Education Collaborative (IPEC) in 2009 and developed four core competencies for interprofessional collaboration.(11)
Values/Ethics for Interprofessional Practice: Work with individuals of other professions to maintain a climate of mutual respect and shared values.
Roles/Responsibilities: Use the knowledge of one’s own role and those of other professions to appropriately assess and address the health care needs of patients and to promote and advance the health of populations.
Interprofessional Communication: Communicate with patients, families, communities, and professionals in health and other fields in a responsive and responsible manner that supports a team approach to the promotion and maintenance of health and the prevention and treatment of disease.
Teams and Teamwork: Apply relationship-building values and principles of team dynamics to perform effectively in different team roles to plan, deliver, and evaluate patient/population-centered care and population health programs and policies that are safe, timely, efficient, effective, and equitable.
When initially released in 2011, the core competencies were proposed under interprofessional education, but the 2016 update emphasizes that they more appropriately represent interprofessional collaboration, aligning with the Nexus vision.
Achieving Interprofessional Practice and Education
Even if one appreciates the beneficial impact of team-based approaches with patient and population health, how does the busy clinician incorporate IPE?
Clinicians practicing within hospital systems (where team-based, multidisciplinary rounds and collaboration already occur) as well as those associated within academic institutions (where IPE programs have leadership support and resources) will find incorporating IPE easier than those in community-based settings. Consider the common designs of interprofessional education modalities.(2)

Some clinical educators will need to be more intentional and persistent about creating IPE opportunities. Some helpful strategies may be gleaned from the National Center’s NexusIPETM toolkit.(9)
Take the time to get to know your IPE ecosystem: Find out what already exists. If there is not much, some clinicians may feel empowered to become champions and advocate for IPE. Academic institutions are often eager to engage with community partners and clinicians.
Build the right IPE team at the right time: Sometimes IPE can seem out of reach due to time constraints and priorities, but establishing a good team can exponentially improve patient experience and outcomes—and it does not have to be complicated. Simply being open to including students from other health professions can be favorable and rewarding. At a previous institution, dental, social work, and couple and family therapy students worked alongside medical students and residents. In addition to medical and mental health conditions, patients benefited from being able to address social determinants of health, and learners benefited both from exposure to experiences they might otherwise not have and the ability to learn with and from each other.
Define your vision and get ready to communicate it: Buy-in from partners or leadership may be needed. Leaning into elements such as the value learners from different professions can add, increased patient satisfaction and ratings, and that, health care professional shortages, practice staffing, and provider recruitment can be improved by helping to fulfill clinical rotation requirements and increasing the workforce candidate pool can be convincing. Barriers may include opportunity cost and potential loss of revenue (e.g., spending more time with students may alter one’s workflow) but may be offset by incentives and stipends offered by sponsoring institutions as well as, for some, the sense of pride and accomplishment that organizations and clinicians play a vital role in training future health professionals. Employing strategies such as One-Minute Preceptor and the Triangle Method of clinical teaching can help with time-limited precepting (but don’t forget the importance of direct observation when precepting).
Conclusion
A common complaint I hear is something along the lines of “why don’t health professionals talk to each other?”. In fairness, we have come a long way (e.g., regardless of your practice setting, you have likely interacted with team-centered care or cooperated with other health professions). Intuitively, we recognize that working together can achieve a goal more efficiently and effectively than laboring alone, and yet health care professions still tend to be siloed. A growing body of evidence suggests that IPE leads to better health care outcomes, particularly in diabetes management, reduced error rates and patient satisfaction for emergency department teams, and care related to domestic violence and mental health.(12,13) Accordingly, by promoting any form of IPE, we can help to break down barriers and place patients first. Unlike my initial experience with interprofessional education, learners and health professionals are increasingly viewing each other as not in conflict but in collaboration toward common outcomes.■
References
(1) National Academy of Medicine. Addressing social determinants of health and health disparities. In: Finkelman EM, McGinnis JM, McClellan MB, et al., eds. Vital Directions for Health & Health Care. National Academies Press; 2016. Accessed May 8, 2024. https://www.ncbi.nlm.nih.gov/books/NBK595183/
(2) Health Professions Accreditors Collaborative. Guidance on developing quality interprofessional education for the health professions. Health Professions Accreditors Collaborative; 2019. Accessed May 8, 2024. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://healthprofessionsaccreditors.org/wp-content/uploads/2019/02/HPACGuidance02-01-19.pdf
(3) World Health Organization. Framework for action on interprofessional education & collaborative practice. 2010. Retrieved April 29, 2024. https://iris.who.int/bitstream/handle/10665/70185/WHO_HRH_HPN_10.3_eng.pdf?sequence=1
(4) Committee on Measuring the Impact of Interprofessional Education on Collaborative Practice and Patient Outcomes, Institute of Medicine. Measuring the impact of interprofessional education on collaborative practice and patient outcomes. National Academies Press; 2015. https://www.ncbi.nlm.nih.gov/books/NBK338360/
(5) Brandt B, Barton A. Getting Started with Interprofessional Practice and Education in Community-Based Settings. J Nurs Educ. 2020;59(5):243-4. doi:10.3928/01484834-20200422-01
(6) Brandt B, Kertz J, Arenson C. National Center for Interprofessional Practice and Education 2023: Reflecting Back, Looking Forward. J of Interprof Care. 2023;37(Sup 1):S4-14.
(7) Institute of Medicine Committe on the Health Professiona Education Summit, Greiner AC, Knebel E, eds. Health professions education: a bridge to quality. National Academy Press; 2003. Accessed May 8, 2024 https://www.ncbi.nlm.nih.gov/books/NBK221528/
(8) Earnest M, Brandt B. Aligning practice redesign and interprofessional education to advance triple aim outcomes. J Interprof Care. 2014;28(6):497-500. doi:10.3109/13561820.2014.933650
(9) Brandt B, Dieter C, Willson A, Pejsa L. Setting the stage for a Transformative NexusIPETM Team: An Introductory Toolkit. National Center for Interprofessional Practice and Education; 2019. Accessed May 8, 2024. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://nexusipe-resource-exchange.s3-us-west-2.amazonaws.com/Introductory%20Toolkit%20-%20National%20Center%2010-18-2019.pdf
(10) Bodenheimer T, Sinsky C. From triple to quadruple aim: care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573-576. doi:10.1370/afm.1713
(11) Interprofessional Education Collaborative. Core competencies for interprofessional collaborative practice: 2016 update. Interprofessional Education Collaborative; 2016. Accessed May 8, 2024. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://ipec.memberclicks.net/assets/2016-Update.pdf
(12) Reeves S, Fletcher S, Barr H, et al. A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Med Teach. 2016;38(7):656-668. doi:10.3109/0142159X.2016.1173663
(13) Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes (update). Cochrane Database Syst Rev. 2013;2013(3):CD002213. Published 2013 Mar 28. doi:10.1002/14651858.CD002213.pub3